Complete Guide for Early Cancer Screening|A Review of Screening Methods for 6 Common Cancers
Compiled by DengYueMed based on publicly available medical guidelines and screening consensus.
Globally, cancer remains one of the most severe threats to human health. Nevertheless, extensive clinical research and public health practices have consistently proven that early screening is one of the most effective measures to reduce cancer mortality.
Leading health authorities universally emphasize that cancer prevention and control should follow the “Four Early Principles” — early prevention, early detection, early diagnosis, and early treatment. Most cancers present a favorable prognosis at early stages, and can be well controlled without interfering with daily life and work.
However, the majority of cancer cases are diagnosed at the advanced stage. The primary reasons lie in the asymptomatic nature of early cancer lesions and insufficient public awareness of proactive screening.
Based on current mainstream medical guidelines and global screening consensus, this article systematically summarizes the standard screening approaches, high-risk populations, and screening intervals for six prevalent cancers, helping individuals and families build scientific and actionable health management strategies.
Key Screening Summary of Six Cancers
| Cancer Type | Primary Screening Method | Recommended Starting Age | Screening Frequency |
|---|---|---|---|
| Lung Cancer | Low-Dose CT (LDCT) | 50 years old | Annual |
| Colorectal Cancer | FIT / Colonoscopy | 40 years old | Annual / As advised by physicians |
| Liver Cancer | Ultrasound + AFP Test | 40 years old (high-risk groups) | Every 6 months |
| Gastric Cancer | Gastroscopy | 45 years old | Risk-based interval |
| Breast Cancer | Ultrasound / Mammography | 45 years old | Every 1–2 years |
| Cervical Cancer | HPV Test | 25 years old | Every 3–5 years |
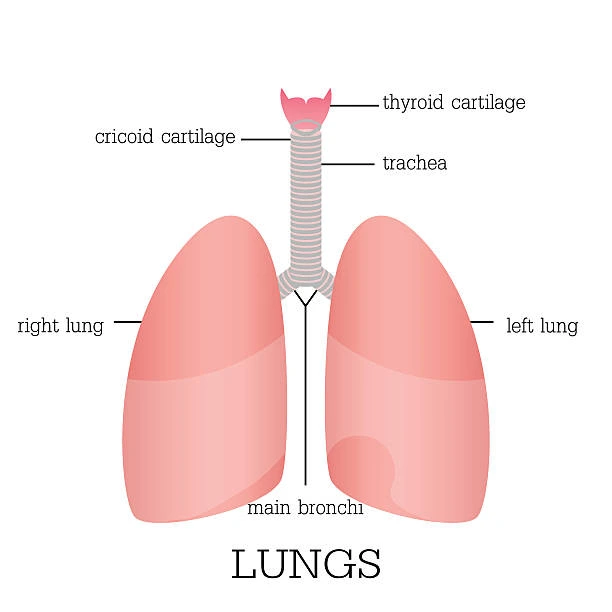
Lung Cancer|A Globally Prevalent Malignancy
✅ Primary Screening Method: Low-Dose Computed Tomography (LDCT)
Recognized globally by the medical community, LDCT is the preferred screening tool for high-risk populations. With low radiation exposure and high accuracy, it can detect tiny early pulmonary lesions far more effectively than conventional chest X-rays.
👥 High-Risk Population (Aged 50–80, meeting any of the following)
- Smoking history of ≥20 pack-years, or quit smoking for less than 5 years; long-term passive smoking for ≥20 years
- Long-term occupational exposure to carcinogens such as radon, arsenic, and chromium
- First-degree or second-degree relatives with lung cancer history, coupled with personal smoking or passive smoking history of ≥15 years
📅 Screening Interval
Individuals with negative screening results for two consecutive years may suspend screening for 2 years. Those with positive findings require annual re-screening.
Colorectal Cancer|Preventable Gastrointestinal Malignancy
✅ Gold Standard Screening: Colonoscopy
Supplementary Screening: Fecal Immunochemical Test (FIT), Multi-target FIT-DNA Test
FIT is non-invasive, cost-effective, and widely accepted for annual primary screening. A positive FIT result requires further confirmatory colonoscopy.
The multi-target FIT-DNA test delivers higher accuracy and is suitable for individuals who prefer non-invasive screening, recommended once every 3 years.
👥 High-Risk Population
- Individuals aged 40 and above for routine screening
- People with a family history of colorectal cancer or intestinal adenoma
- Patients with chronic enteritis, persistent fecal occult blood positivity, or chronic intestinal diseases
Suggestion: Individuals with a family history should start screening 10 years earlier than the youngest affected family member.
Liver Cancer|Highly Occult, Usually Diagnosed at Advanced Stages
✅ Standard Screening Combination: Liver Ultrasound + Alpha-Fetoprotein (AFP) Test
Ultrasound is non-invasive, radiation-free, cost-efficient, and widely applicable for observing liver morphology, structure, and space-occupying lesions. AFP serves as a core tumor marker for liver cancer. This combined approach is the internationally accepted primary screening solution suitable for most populations.
Enhanced CT or gadoxetic acid-enhanced MRI is recommended for further diagnosis and staging if abnormal lesions are detected.
👥 High-Risk Population
- Patients with liver cirrhosis caused by various liver diseases
- Individuals aged 40 and above with chronic hepatitis B or C infection
- People with long-term alcohol abuse, frequent intake of smoked, pickled or moldy food, chronic fatigue and late-night working habits
Tips: Liver cancer is not directly hereditary, but presents obvious familial aggregation. Family members of patients are advised to prioritize screening.
Gastric Cancer|Highly Prevalent Among People with Unhealthy Dietary Habits
✅ Gold Standard Screening: Gastroscopy + Pathological Biopsy
Core Auxiliary Screening: Helicobacter Pylori (Hp) Urea Breath Test
Helicobacter pylori is a major risk factor for gastric cancer. Screening for Hp is prioritized for residents in high-incidence areas. Single serum biomarker testing is not recommended for independent screening due to insufficient accuracy.
👥 High-Risk Population (Aged 45+, meeting any of the following)
- Residents in high-incidence areas of gastric cancer and Hp-positive individuals
- Patients with chronic atrophic gastritis, gastric ulcers, gastric polyps and other precancerous gastric conditions
- Individuals with first-degree relatives diagnosed with gastric cancer
- People with long-term high-salt diets, frequent consumption of pickled foods, heavy smoking and excessive drinking
Breast Cancer|The Most Prevalent Malignancy in Females
✅ Tiered Screening Recommendations
For average-risk women: Breast ultrasound is the preferred primary screening method, which adapts to the characteristics of dense breast tissue in Asian women and is safe for pregnant and lactating women.
For high-risk individuals and women with dense breasts: Combined screening of breast ultrasound and mammography is recommended.
For genetically high-risk populations: Breast MRI can be adopted as required.
👥 High-Risk Population & Screening Age
Average-risk women: start screening at 45 years old; high-risk women may begin screening at 40 years old.
- Individuals with a family history of breast or ovarian cancer and BRCA1/BRCA2 pathogenic mutations
- Women with early menarche, late menopause, or a history of atypical breast hyperplasia
- Women with no breastfeeding experience, advanced childbearing age, or long-term hormone replacement therapy
Cervical Cancer|The Only Preventable and Interceptable Malignancy
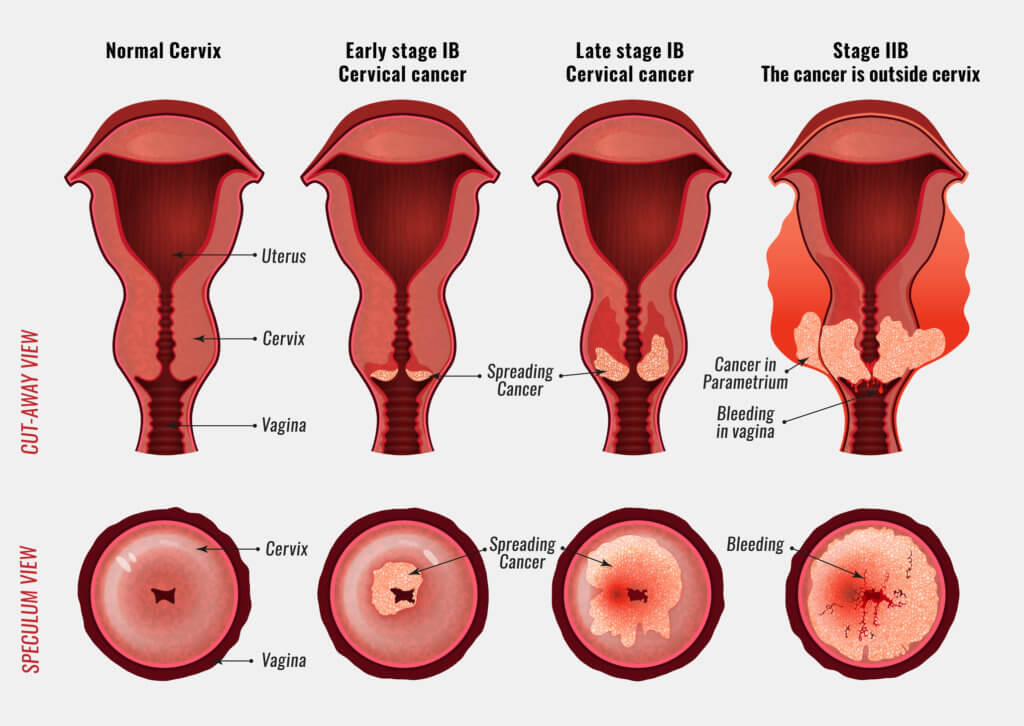
✅ Primary Screening: HPV Nucleic Acid Test
Golden Combined Screening: HPV Test + TCT Cytological Test
The HPV test offers high sensitivity, while the TCT test provides high specificity. Combined screening can detect the vast majority of early cervical lesions and precancerous lesions. Visual inspection methods are optional for primary screening in medically under-resourced regions.
📅 Routine Screening Interval (Women aged 25–64)
- Single HPV test: every 5 years
- Combined HPV & TCT test: every 5 years
- Single TCT test: every 3 years
Important Reminder: Regular screening is still required even after HPV vaccination. Women with early sexual activity, multiple sexual partners, smoking habits or immune deficiency need earlier and more frequent screening. Women over 65 without regular screening history should continue screening.
Conclusion
The core of cancer prevention and control lies in early prevention and regular screening, rather than late-stage treatment.
Scientific and periodic screening represents one of the most cost-effective approaches to long-term health management. Proactive screening is far more reliable than relying on physical symptoms.
Establishing long-term screening awareness for yourself and your family is critical to reducing the risk of severe diseases.
Related Posts
- KRAS-Mutant Non-Small Cell Lung Cancer Treatment Advances: From G12C Inhibitors to Pan-RAS Therapies
- Mapping China's RAS Pipeline Landscape: From “Undruggable” Target to a New Frontier in Oncology Innovation
- April 2026 Breakthroughs in Cancer Treatment: 26 New Projects Launched, Advances in Immunotherapy and Precision Targeting