How Is a Pituitary Tumor Treated? A Comprehensive Guide to Surgery, Medication, and Radiation Therapy
Pituitary tumors are among the most common benign intracranial tumors, accounting for approximately 10–15% of all brain tumors.
Although most pituitary tumors grow slowly and are noncancerous, some can produce excessive hormones or compress nearby structures such as the optic nerves, leading to vision problems, endocrine disorders, headaches, infertility, and a reduced quality of life.
Fortunately, advances in endocrinology, neurosurgery, imaging technologies, and radiation oncology have dramatically improved treatment outcomes over the past two decades. Today, many patients achieve excellent long-term disease control through medication, minimally invasive surgery, radiation therapy, or individualized combination treatment.
This article explains the major treatment options for pituitary tumors, discusses how treatment differs among various tumor types, and outlines the latest multidisciplinary management strategies based on current international clinical guidelines.
What Is a Pituitary Tumor?
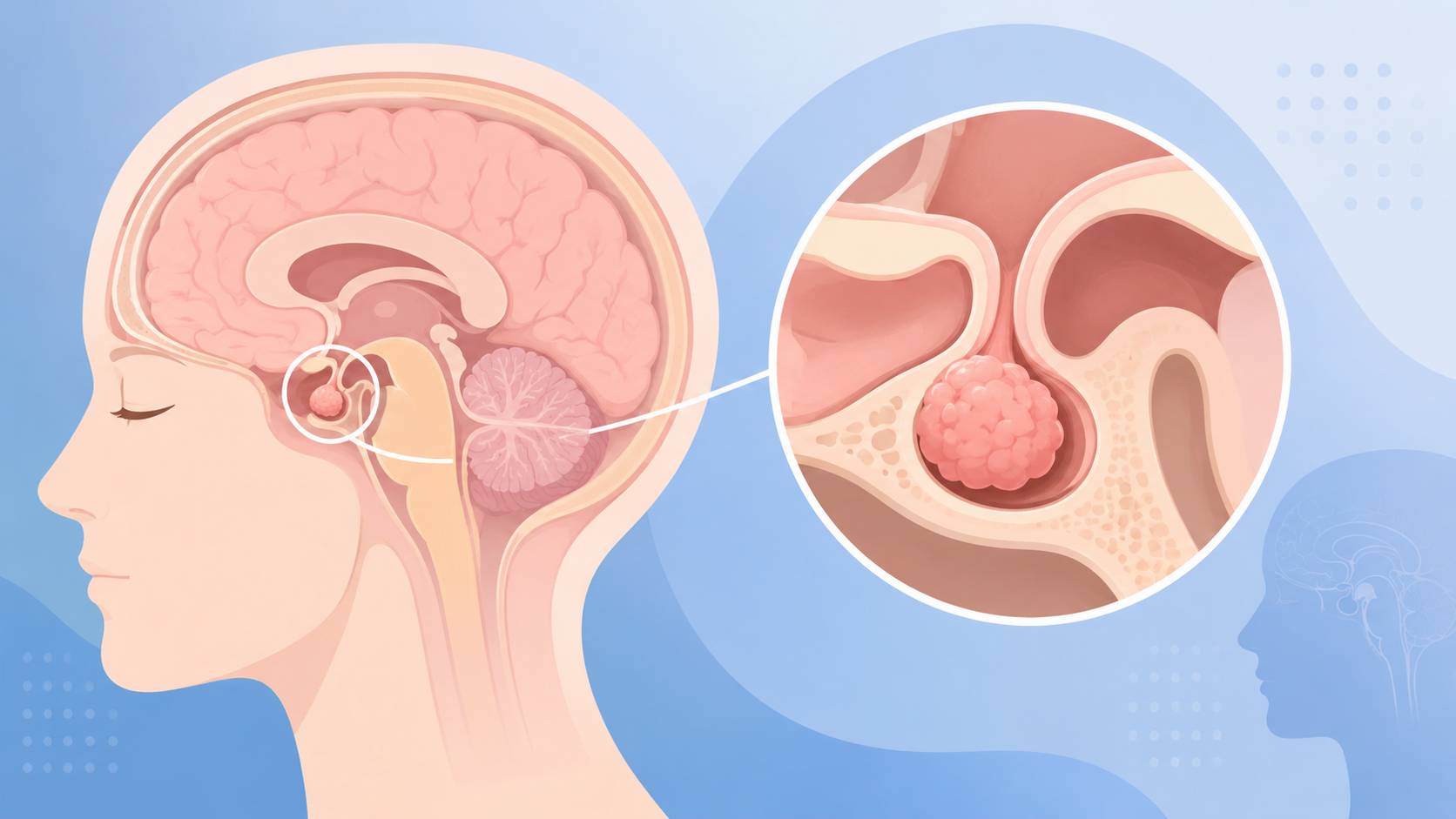
The pituitary gland is a pea-sized endocrine organ located at the base of the brain beneath the hypothalamus. It is often called the body’s “master endocrine gland” because it regulates hormone production throughout the body.
Pituitary hormones influence numerous physiological functions, including:
- Thyroid function
- Adrenal gland activity
- Reproductive hormones
- Growth and development
- Lactation
- Water balance
- Metabolism
A pituitary tumor, also known as a pituitary adenoma, develops when pituitary cells begin growing abnormally.
Most pituitary adenomas are benign and slow growing. However, depending on their size and hormone-producing ability, they can cause significant health problems.
Pituitary tumors are generally classified into two major categories:
Functioning Pituitary Adenomas
These tumors actively produce excessive hormones.
The major subtypes include:
- Prolactinoma
- Growth hormone (GH)-secreting adenoma
- ACTH-secreting adenoma (Cushing’s disease)
- TSH-secreting adenoma
Because these tumors disrupt the body’s hormonal balance, they often require active treatment even when relatively small.
Non-Functioning Pituitary Adenomas (NFPA)
Non-functioning adenomas do not produce biologically active hormones.
Instead, symptoms usually occur because the tumor gradually enlarges and compresses surrounding structures, including:
- The optic chiasm
- Normal pituitary tissue
- Cranial nerves
- Adjacent brain structures
Large tumors may result in:
- Persistent headaches
- Blurred vision
- Loss of peripheral vision
- Fatigue
- Hormone deficiencies
- Pituitary insufficiency
Treatment decisions depend on both tumor size and symptom severity.
Which Pituitary Tumors Require Treatment?
Not every pituitary tumor requires immediate intervention.
Small pituitary adenomas discovered incidentally during MRI examinations may remain stable for years without causing symptoms.
For carefully selected patients, regular observation with periodic MRI scans and hormone testing may be sufficient.
However, treatment is generally recommended when one or more of the following conditions are present:
- Tumor diameter greater than 10 mm (macroadenoma)
- Progressive tumor enlargement
- Compression of the optic nerves or optic chiasm
- Visual impairment or visual field defects
- Excessive hormone secretion
- Headaches caused by tumor compression
- Pituitary apoplexy (acute hemorrhage or infarction)
- Compression leading to impaired normal pituitary function
The decision to begin treatment should always be based on a comprehensive evaluation performed by experienced endocrinologists and neurosurgeons, taking into account:
- MRI findings
- Hormone laboratory tests
- Visual field examinations
- Neurological symptoms
- Patient age
- Overall health status
Main Treatment Options for Pituitary Tumors
The primary treatment options for pituitary tumors include medication, endoscopic transsphenoidal surgery, radiation therapy, and combination therapy.
The most appropriate treatment depends on several factors, including:
- Tumor type
- Tumor size
- Hormone secretion status
- Whether the tumor compresses surrounding structures
- Patient age
- General health condition
- Previous treatment history
An individualized treatment plan developed by a multidisciplinary team (MDT) generally provides the best long-term outcomes.
1. Medication
Medication is considered the first-line treatment for certain hormone-secreting pituitary tumors, particularly prolactinomas.
The goals of medical therapy include:
- Suppressing excessive hormone secretion
- Shrinking the tumor
- Relieving symptoms
- Preserving normal pituitary function
- Delaying or avoiding surgery when appropriate
Because different pituitary tumors produce different hormones, treatment varies according to tumor subtype.
Prolactinoma
Prolactinomas are the most common functioning pituitary adenomas and usually respond extremely well to dopamine agonists.
The preferred medications include:
- Cabergoline
- Bromocriptine
Cabergoline is generally considered the preferred first-line agent because it:
- Produces higher normalization rates of prolactin
- Shrinks tumors more effectively
- Requires less frequent dosing
- Causes fewer gastrointestinal side effects
In many patients, dopamine agonists can reduce prolactin levels to normal and significantly decrease tumor size, eliminating the need for surgery.
Growth Hormone-Secreting Adenoma
Growth hormone-producing adenomas cause acromegaly in adults and gigantism in children.
When surgery cannot completely remove the tumor or hormone levels remain elevated, several medications are available.
Common options include:
- Octreotide
- Lanreotide
- Pasireotide
- Pegvisomant
These medications help:
- Lower growth hormone (GH) levels
- Normalize insulin-like growth factor-1 (IGF-1)
- Improve symptoms
- Reduce cardiovascular complications
- Slow disease progression
For selected patients, combination medical therapy may provide better hormonal control.
ACTH-Secreting Adenoma
ACTH-producing tumors cause Cushing’s disease, characterized by excessive cortisol production.
Although surgery remains the preferred treatment, medications play an important role when:
- Surgery is not possible
- Residual tumor remains
- Disease recurs
- Cortisol remains uncontrolled after surgery
Available medications include:
- Pasireotide
- Osilodrostat
- Levoketoconazole (available in selected countries and regions)
These therapies reduce cortisol production and improve symptoms such as:
- Hypertension
- Diabetes
- Weight gain
- Muscle weakness
- Osteoporosis
TSH-Secreting Adenoma
TSH-secreting pituitary adenomas are rare.
Medical therapy may include somatostatin analogs before surgery to improve hormone control and reduce tumor volume.
However, definitive treatment usually involves surgery.
Advantages of Medical Therapy
Compared with surgery, medication offers several advantages for selected patients:
- Non-invasive treatment
- Preservation of pituitary function
- Effective hormone control
- Tumor shrinkage
- Improved quality of life
- Reduced surgical risks
However, long-term treatment often requires regular hormone monitoring and MRI examinations.
2. Endoscopic Transsphenoidal Surgery
For many pituitary tumors, endoscopic endonasal transsphenoidal surgery has become the international standard of care.
Instead of opening the skull, surgeons access the pituitary gland through the nasal cavity and sphenoid sinus using a high-definition endoscope.
This minimally invasive approach has largely replaced traditional microscopic surgery at major pituitary centers worldwide.
Advantages of Endoscopic Surgery
Compared with conventional craniotomy, endoscopic transsphenoidal surgery offers numerous advantages:
- No external incision
- No opening of the skull
- Better visualization of the surgical field
- Greater preservation of normal pituitary tissue
- Reduced blood loss
- Less postoperative pain
- Faster recovery
- Shorter hospitalization
- Lower complication rates
High-definition endoscopic imaging also improves visualization around critical structures such as:
- Internal carotid arteries
- Optic nerves
- Cavernous sinus
- Pituitary stalk
This allows surgeons to safely remove more tumor tissue while minimizing neurological injury.
When Is Surgery Recommended?
Surgery is commonly recommended for patients with:
- Non-functioning macroadenomas
- Tumors compressing the optic nerves
- Progressive visual loss
- Growth hormone-secreting adenomas
- ACTH-secreting adenomas
- TSH-secreting adenomas
- Pituitary apoplexy
- Tumors that respond poorly to medication
In experienced pituitary centers, complete tumor removal can often be achieved for appropriately selected patients.
Technological Advances
Modern pituitary surgery continues to improve through several technological innovations, including:
- High-definition endoscopy
- Three-dimensional visualization
- Neuronavigation systems
- Intraoperative MRI
- Fluorescence-guided surgery
- Intraoperative hormone monitoring
These technologies improve both surgical precision and long-term treatment outcomes.
3. Radiation Therapy
Radiation therapy plays an important role when surgery cannot completely eliminate the tumor or when disease recurs.
It is generally recommended for patients with:
- Residual tumor after surgery
- Recurrent pituitary adenomas
- Tumors invading the cavernous sinus
- Patients unsuitable for repeat surgery
- Persistent hormone hypersecretion despite other treatments
Modern radiation techniques are significantly more precise than conventional radiotherapy performed decades ago.
Stereotactic Radiosurgery (SRS)
Stereotactic radiosurgery delivers highly focused radiation to the tumor while minimizing damage to surrounding healthy tissues.
Common technologies include:
- Gamma Knife
- CyberKnife
SRS is particularly suitable for:
- Small residual tumors
- Recurrent pituitary adenomas
- Tumors located away from the optic nerves
- Patients unable to undergo additional surgery
Benefits include:
- High precision
- Outpatient treatment
- Minimal recovery time
- Excellent long-term tumor control
- Low complication rates
Hormone normalization may require months or even years after treatment, making long-term follow-up essential.
Conventional Fractionated Radiotherapy
Fractionated radiotherapy remains valuable for patients with:
- Large residual tumors
- Tumors close to the optic apparatus
- Extensive cavernous sinus invasion
- Complex postoperative disease
Rather than delivering radiation in a single session, treatment is divided into multiple smaller doses over several weeks, reducing the risk of radiation-induced injury to nearby structures.
4. Combination Therapy
Increasingly, patients benefit from a multidisciplinary treatment strategy that combines multiple therapies.
Common treatment combinations include:
- Medication + Surgery
- Surgery + Radiation Therapy
- Medication + Radiation Therapy
- Surgery + Medication + Radiation Therapy
Combination therapy may:
- Improve hormone normalization
- Increase long-term tumor control
- Reduce recurrence risk
- Preserve pituitary function
- Improve overall quality of life
The optimal sequence of treatments should always be individualized according to tumor characteristics and patient-specific factors.
3. Radiation Therapy
Radiation therapy is generally recommended for patients with:
- Residual tumor after surgery
- Tumors that cannot be completely removed
- Recurrent pituitary tumors
- Patients who are not suitable candidates for repeat surgery
Common radiation techniques include:
Stereotactic Radiosurgery (SRS)
This includes technologies such as:
- Gamma Knife
- CyberKnife
SRS is particularly suitable for:
- Small residual tumors
- Lesions located away from critical neural structures
Its advantages include:
- High precision
- Single-session or limited-session treatment
- Minimal damage to surrounding healthy tissue
Conventional Fractionated Radiotherapy
This approach is generally used for:
- Larger residual tumors
- Patients who are not suitable candidates for stereotactic radiosurgery
- Tumors located close to the optic nerves or optic chiasm
Although conventional radiotherapy requires multiple treatment sessions, it remains an effective option for long-term tumor control when radiosurgery is not appropriate.
4. Combination Therapy
An increasing number of patients benefit from multidisciplinary combination therapy to achieve better long-term outcomes.
Common treatment combinations include:
- Medication + Surgery
- Surgery + Radiation Therapy
- Medication + Radiation Therapy
- Surgery + Medication + Radiation Therapy
Combination therapy may help:
- Improve hormone control
- Reduce recurrence risk
- Preserve pituitary function
- Improve long-term quality of life
- Achieve better overall survival in selected patients
How Is Treatment Selected for Different Types of Pituitary Tumors?
Different pituitary tumors require different treatment strategies.
| Pituitary Tumor Type | Preferred Treatment |
|---|---|
| Prolactinoma | Medication (Dopamine Agonists) |
| Growth Hormone-Secreting Adenoma | Surgery ± Medication |
| ACTH-Secreting Adenoma | Primarily Surgery |
| TSH-Secreting Adenoma | Primarily Surgery |
| Non-Functioning Pituitary Adenoma | Observation or Surgery |
Treatment decisions should take multiple factors into consideration, including:
- Tumor size
- Cavernous sinus invasion
- Hormone levels
- Patient age
- Overall medical condition
- Presence of visual impairment
- Patient preferences
- Surgical risk
- Expected long-term endocrine function
Because pituitary tumors involve both neurosurgical and endocrine management, treatment is best planned by a multidisciplinary team (MDT) consisting of:
- Neurosurgeons
- Endocrinologists
- Radiation oncologists
- Neuroradiologists
- Pathologists
- Neuro-ophthalmologists
What Is the Prognosis for Patients with Pituitary Tumors?
Fortunately, most pituitary tumors are benign, and modern treatment has significantly improved long-term outcomes.
Overall prognosis depends on several factors, including:
- Tumor type
- Hormone secretion status
- Tumor size
- Extent of surgical removal
- Response to medication
- Whether recurrence occurs
For many patients:
- Prolactinomas respond well to dopamine agonists.
- Growth hormone and ACTH-secreting tumors often achieve hormonal remission after surgery.
- Non-functioning adenomas usually have excellent long-term survival after complete resection.
Regular follow-up remains essential because some tumors may recur years after initial treatment.
Long-Term Follow-Up After Treatment
Patients are usually advised to undergo regular monitoring after treatment.
Typical follow-up includes:
- Brain MRI
- Pituitary hormone testing
- Visual field examinations
- Endocrine function assessment
- Medication adjustment if necessary
The frequency of follow-up depends on:
- Tumor subtype
- Surgical outcome
- Hormone status
- Presence of residual tumor
- Previous radiation therapy
Long-term surveillance helps detect recurrence early and optimize endocrine replacement therapy when needed.
Frequently Asked Questions (FAQ)
Can pituitary tumors be cured?
Many pituitary tumors can be completely removed through surgery or effectively controlled with medication. Long-term remission is common, particularly for small tumors diagnosed early.
Is surgery always necessary?
No.
Many prolactinomas can be successfully treated with medication alone, while some small non-functioning pituitary adenomas may only require regular observation.
Are pituitary tumors cancerous?
The vast majority of pituitary tumors are benign (pituitary adenomas). Pituitary carcinoma is extremely rare.
Will hormone levels return to normal after treatment?
Many patients experience normalization of hormone levels following successful treatment, although some may require lifelong hormone replacement therapy if normal pituitary function is affected.
Future Perspectives
Advances in pituitary tumor management continue to improve patient outcomes.
Current research focuses on:
- More precise molecular classification
- AI-assisted MRI analysis
- Improved endoscopic surgical navigation
- Novel targeted therapies
- Precision endocrine management
- Personalized follow-up strategies
These innovations are expected to further increase cure rates while minimizing treatment-related complications.
Conclusion
Today, most patients with pituitary tumors can achieve excellent disease control through medication, minimally invasive surgery, radiation therapy, or a combination of these approaches.
Because treatment strategies vary considerably according to tumor subtype, hormone secretion, and tumor size, patients should work closely with experienced specialists to develop an individualized treatment plan.
Early diagnosis, standardized multidisciplinary treatment, and long-term follow-up remain the keys to preserving endocrine function, protecting vision, reducing recurrence, and improving overall quality of life.
About DengYueMed
Hong Kong DengYue Pharmaceutical Limited (DengYueMed) is a global pharmaceutical distributor specializing in innovative medicines, oncology therapies, rare disease treatments, and international pharmaceutical supply solutions.
We connect healthcare providers, pharmacies, distributors, and compliant partners with trusted pharmaceutical sourcing services and access to innovative medicines worldwide.
Disclaimer
This article is intended for educational and informational purposes only and should not replace professional medical advice, diagnosis, or treatment. Patients should always consult qualified healthcare professionals regarding diagnosis and treatment decisions.