Can TCR-T Become the Next Breakthrough for Advanced Head and Neck Cancer?
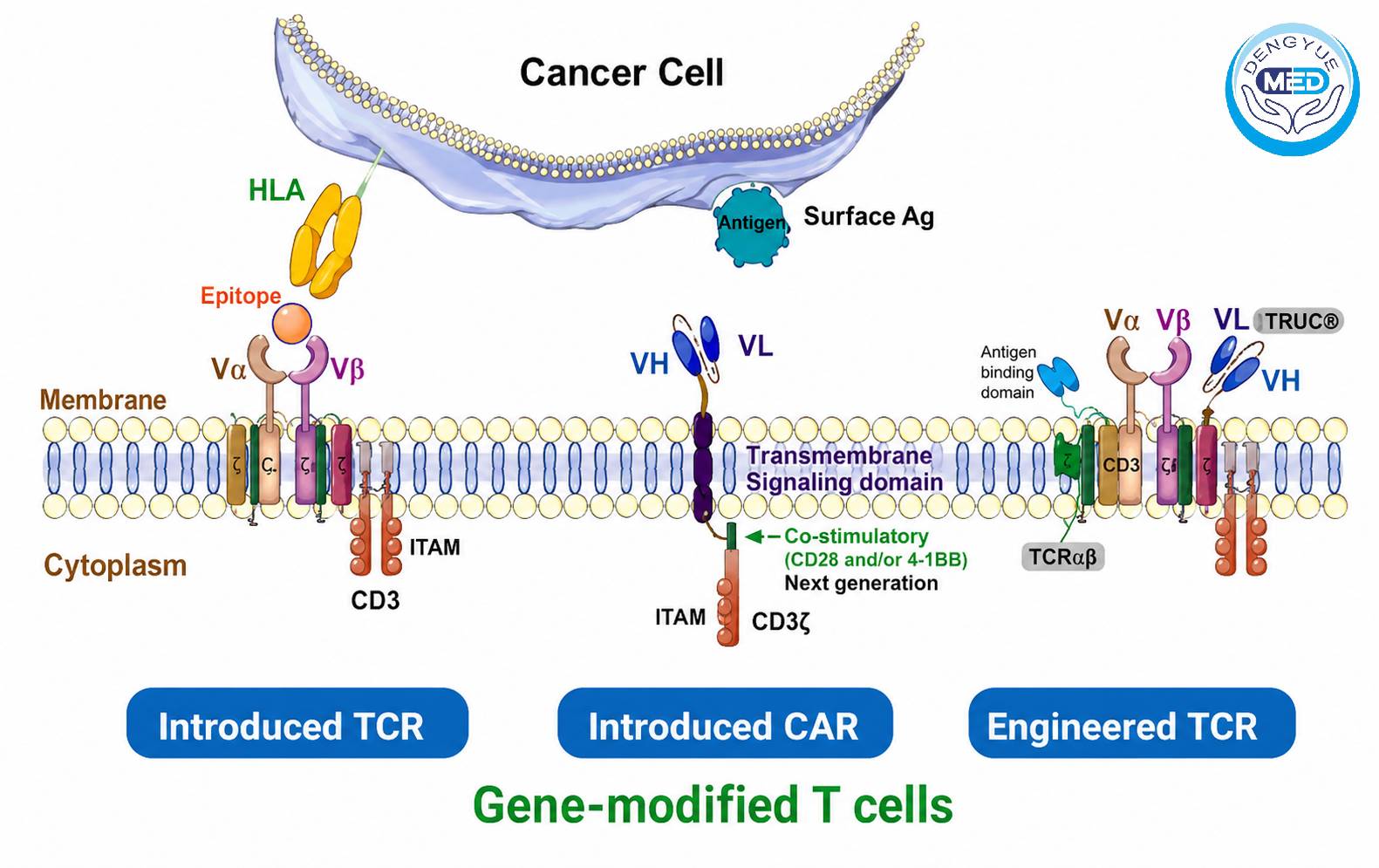
Table of Contents
- Introduction
- Significant Unmet Needs Remain in Advanced HNSCC
- What Is TCR-T Therapy?
- Why Is TCR-T Better Suited for Solid Tumors?
- Latest Clinical Progress
- Current Challenges
- Future Perspectives
- Conclusion
- Frequently Asked Questions
Introduction
Immunotherapy has fundamentally transformed the treatment landscape for multiple cancers over the past decade. For patients with recurrent or metastatic head and neck squamous cell carcinoma (HNSCC), immune checkpoint inhibitors targeting the PD-1/PD-L1 pathway have become an important component of first-line therapy.
Despite these advances, durable clinical responses remain limited. Many patients eventually experience primary resistance, acquired resistance, or disease progression after immunotherapy.
As researchers continue searching for more effective treatment strategies, cellular immunotherapy has rapidly emerged as one of the most exciting areas of oncology innovation.
Among these technologies, T Cell Receptor-Engineered T Cell Therapy (TCR-T) has attracted significant attention because it can recognize intracellular tumor antigens that are inaccessible to conventional CAR-T therapy.
Unlike CAR-T cells, which are limited to recognizing proteins expressed on the surface of cancer cells, TCR-T cells recognize peptide fragments presented by Human Leukocyte Antigen (HLA) molecules, dramatically expanding the number of potential therapeutic targets.
This unique biological characteristic has made TCR-T one of the leading candidates for overcoming many of the barriers that have limited cellular therapy in solid tumors.
In this article, Hong Kong DengYue Pharmaceutical Limited (DengYueMed) reviews the latest scientific evidence regarding TCR-T therapy for advanced HNSCC, including its mechanism of action, clinical development, advantages, current limitations, and future prospects.
Significant Unmet Needs Remain in Advanced HNSCC
Head and neck squamous cell carcinoma includes malignancies arising from the:
- Oral cavity
- Oropharynx
- Hypopharynx
- Larynx
Globally, more than 900,000 new cases are diagnosed each year, making HNSCC one of the most common solid malignancies worldwide.
For patients with localized disease, multidisciplinary treatment usually consists of:
- Surgery
- Radiotherapy
- Chemotherapy
- Concurrent chemoradiotherapy
However, treatment options become considerably more limited once disease recurs or metastasizes.
Current standard systemic therapies include:
- PD-1 inhibitors
- EGFR-targeted therapy
- Platinum-based chemotherapy
- Combination immunotherapy
The landmark KEYNOTE-048 trial established pembrolizumab-based therapy as an international first-line standard for recurrent or metastatic HNSCC.
Nevertheless, important clinical challenges remain:
- Limited objective response rates
- Development of acquired resistance
- Short progression-free survival in many patients
- Poor long-term survival for advanced disease
Consequently, identifying more durable and personalized immunotherapeutic approaches has become one of the highest priorities in head and neck cancer research.
What Is TCR-T Therapy?
T Cell Receptor-Engineered T Cell Therapy (TCR-T) is a form of adoptive cellular immunotherapy that genetically modifies a patient’s own T lymphocytes to recognize tumor-specific antigens.
Unlike conventional immunotherapy, which stimulates naturally occurring immune responses, TCR-T directly engineers immune cells with highly specific tumor-recognizing receptors.
The treatment process generally involves several steps.
Step 1. Collection of T Cells
Peripheral blood is collected from the patient through leukapheresis.
T lymphocytes are then isolated for laboratory processing.
Step 2. Genetic Engineering
Scientists introduce genes encoding tumor-specific T-cell receptors into the patient’s T cells using viral vectors or other gene-transfer technologies.
These engineered receptors allow the modified T cells to recognize selected tumor-associated antigens.
Step 3. Cell Expansion
The engineered T cells are expanded under controlled laboratory conditions until hundreds of millions or even billions of therapeutic cells are produced.
Step 4. Patient Conditioning
Before infusion, many patients receive lymphodepleting chemotherapy.
This conditioning treatment creates a more favorable immune environment that supports T-cell expansion after infusion.
Step 5. TCR-T Cell Infusion
The engineered cells are infused back into the patient intravenously.
Once inside the body, they migrate toward tumor tissues and begin recognizing cancer cells carrying the target antigen.
Step 6. Tumor Cell Elimination
After recognizing tumor-associated peptide-HLA complexes, TCR-T cells become activated and destroy malignant cells through multiple cytotoxic mechanisms while also generating long-term immune surveillance.
Unlike monoclonal antibodies or conventional chemotherapy, TCR-T functions as a living therapy capable of expanding and persisting within the patient for extended periods.
Latest Clinical Progress of TCR-T in Advanced HNSCC
Current research on TCR-T therapy for advanced HNSCC mainly focuses on several promising therapeutic targets.
HPV16 E6/E7-Specific TCR-T
This is currently the most active area of TCR-T research in head and neck cancer.
Potential indications include:
- HPV-positive oropharyngeal cancer
- HPV-associated recurrent HNSCC
- Metastatic HPV-positive HNSCC
Early Phase I/II clinical studies have reported:
- Objective responses in selected patients
- Durable responses lasting more than one year in some cases
- Generally manageable safety profiles
Because HPV viral proteins are foreign antigens that are continuously expressed by tumor cells while absent from normal tissues, they are considered ideal TCR-T targets.
MAGE-A4 TCR-T
MAGE-A4 belongs to the cancer-testis antigen (CTA) family and is characterized by:
- Expression in multiple solid tumors
- Minimal expression in healthy adult tissues
- Strong immunogenicity
- High specificity for engineered TCR therapy
Several biotechnology companies are currently evaluating MAGE-A4-specific TCR-T therapies across multiple solid tumors, including HNSCC.
NY-ESO-1 TCR-T
NY-ESO-1 is another classic cancer-testis antigen.
Although its expression frequency in HNSCC is relatively low compared with sarcoma or melanoma, antigen-positive patients may still benefit from TCR-T therapy.
Multiple early clinical trials continue to evaluate its potential.
Personalized Neoantigen TCR-T
One of the most exciting directions in precision oncology is personalized neoantigen-specific TCR-T.
Using technologies such as:
- Whole-exome sequencing (WES)
- RNA sequencing
- AI-assisted neoantigen prediction
- Single-cell sequencing
Researchers can identify unique tumor mutations for each patient and engineer individualized TCRs capable of recognizing those mutations.
This strategy may significantly improve treatment specificity while minimizing off-target toxicity.
Challenges Facing TCR-T Therapy
Despite its enormous promise, several important challenges remain.
1. HLA Restriction
Unlike CAR-T therapy, TCR recognition depends on Human Leukocyte Antigen (HLA).
This means:
- Patients must possess compatible HLA types.
- A single TCR-T product cannot treat all patients.
- Different populations require different TCR designs.
Expanding HLA coverage remains an important research priority.
2. Tumor Immune Escape
Tumor cells may evade immune recognition through several mechanisms, including:
- Downregulation of HLA molecules
- Loss of target antigen expression
- Activation of immune suppressive pathways
These mechanisms may reduce the effectiveness of TCR-T therapy over time.
3. Immunosuppressive Tumor Microenvironment
Advanced HNSCC often contains a highly suppressive tumor microenvironment rich in:
- Regulatory T cells (Tregs)
- Myeloid-derived suppressor cells (MDSCs)
- Transforming Growth Factor-β (TGF-β)
- Interleukin-10 (IL-10)
These factors inhibit T-cell activation and persistence.
Researchers are therefore investigating combination approaches such as:
- TCR-T + PD-1 inhibitors
- TCR-T + IL-2 variants
- TCR-T + TGF-β inhibitors
- TCR-T + oncolytic viruses
4. Manufacturing Complexity
Current TCR-T products remain personalized therapies requiring:
- Patient leukapheresis
- Genetic engineering
- Cell expansion
- Quality control testing
- Cryopreservation
- Individualized logistics
Consequently, manufacturing remains expensive and time-consuming.
Future “off-the-shelf” allogeneic TCR-T platforms may significantly improve accessibility.
Can TCR-T Become the Next Breakthrough for Advanced HNSCC?
Current evidence suggests considerable potential.
Compared with conventional therapies, TCR-T offers several unique advantages:
- Recognition of intracellular tumor antigens
- Broad applicability to solid tumors
- Strong potential for HPV-associated HNSCC
- Long-term immune surveillance
- Compatibility with combination immunotherapy
Future advances are expected in several areas:
- Discovery of novel tumor-specific antigens
- AI-assisted TCR screening
- Improved gene-editing technologies
- Universal allogeneic TCR-T products
- Combination treatment strategies
- Biomarker-guided patient selection
As these technologies mature, TCR-T could become one of the cornerstone treatments for advanced head and neck cancer.
Future Outlook
The next generation of cellular immunotherapy will likely integrate multiple innovative technologies.
Potential future directions include:
- Personalized TCR-T
- CRISPR-enhanced TCR engineering
- Multi-target TCR-T
- Cytokine-armored TCR-T
- TCR-T combined with ADCs
- TCR-T combined with bispecific antibodies
- TCR-T combined with immune checkpoint inhibitors
Artificial intelligence, spatial transcriptomics, and single-cell sequencing are expected to accelerate the identification of optimal tumor antigens while improving therapeutic precision.
Conclusion
Patients with advanced head and neck squamous cell carcinoma continue to face high recurrence rates, treatment resistance, and limited long-term survival.
By recognizing intracellular tumor antigens and targeting virus-associated proteins and personalized neoantigens, TCR-T therapy represents one of the most promising innovations in solid tumor immunotherapy.
Although important challenges—including HLA restriction, manufacturing complexity, and immune escape—remain, rapid advances in gene engineering, artificial intelligence, and precision medicine are accelerating the clinical development of TCR-T.
Looking ahead, TCR-T is expected to complement PD-1 inhibitors, targeted therapies, antibody-drug conjugates (ADCs), and other next-generation immunotherapies, helping usher in a new era of personalized treatment for advanced HNSCC.
About DengYueMed
Hong Kong DengYueMed is committed to tracking global advances in oncology, rare diseases, innovative biologics, antibody-drug conjugates (ADCs), cell therapies, and precision medicine.
We provide healthcare professionals, hospitals, pharmacies, and compliant international partners with timely pharmaceutical insights, cross-border medicine information, and updates on emerging treatment technologies to support global access to innovative therapies.
Disclaimer
This article is intended for educational and scientific information exchange only. It does not constitute medical advice, diagnosis, or treatment recommendations. Patients should consult qualified healthcare professionals before making any treatment decisions.
Related Posts
- ADC Landscape in Head and Neck Cancer: Latest Advances in HER3, EGFR, B7-H3, and Other Emerging Targets
- Why Do Many Solid Tumor Treatments Still Rely on Infusion Therapy? The 2026 Landscape of Oncology Injection-Based Treatments
- How Is a Pituitary Tumor Treated? A Comprehensive Guide to Surgery, Medication, and Radiation Therapy